This article is a part of the The Law, Economics, and Policy of the COVID-19 Pandemic symposium.
[TOTM: The following is part of a blog series by TOTM guests and authors on the law, economics, and policy of the ongoing COVID-19 pandemic. The entire series of posts is available here.
This post is authored by Julian Morris, (Director of Innovation Policy, ICLE).]
SARS-CoV2, the virus that causes COVID-19, is now widespread in the population in many countries, including the US, UK, Australia, Iran, and many European countries. Its prevalence in other regions, such as South Asia, much of South America, and Africa, is relatively unknown. The failure to contain the virus early on has meant that more aggressive measures are now necessary in order to avoid overwhelming healthcare systems, which would cause unacceptable levels of mortality. (Sadly, Italy’s health system has already been overwhelmed, forcing medical practitioners to engage in the most awful triage decisions.) Many jurisdictions, ranging from cities to entire countries, have chosen to implement mandatory lockdowns. These will likely have the desired effect of slowing transmission in the short term, but they cannot be maintained indefinitely. The challenge going forward is how to contain the spread of the virus without destroying the economy.
In this post I will outline the elements of a proposal that I hope might do that. (I’ve been working on this for about a week and in the meantime some of the ideas have been advanced by others. E.g. this and this. Great minds clearly think alike.)
1. Identify those who have had COVID-19 and have recovered — and allow them to go back to work
While there are some reports of people who have had COVID-19 becoming reinfected, this seems to be very rare (a recent primate study implies reinfection is impossible) and the alleged cases may have been a result of false negative tests followed by relapse by patients. The general presumption is that having the disease is likely to confer immunity for several months at least. Moreover, people with immunity who no longer show symptoms of the disease are very unlikely to transmit the disease. Allowing those people to go back to work will lessen the burden of the lockdown without appreciably increasing the risk of infection
One group of such people is readily identifiable, though small: Those who tested positive for COVID-19 and subsequently recovered. Those people should be permitted to go back to work immediately.
2. Where possible, test, trace, treat, isolate
The town of Vo in Northern Italy, the site of the first death in the country from COVID-19, appears to have stopped the disease from spreading in about three weeks. It did so through a combination of universal testing, two weeks of strict lockdown, and quarantine of cases. Could this be replicated elsewhere?
Vo has a population of 3,300, so universal testing was not the gargantuan exercise it would be in, say, the continental US. Some larger jurisdictions have had similar success without resorting to universal testing and lockdown. South Korea managed to contain the spread of SARS-CoV2 relatively quickly through a combination of: social distancing (including closing schools and restricting large gatherings), testing anyone who had COVID-19 symptoms (and increasingly those without symptoms), tracing and testing of those who had contact with those symptomatic individuals, treating those with severe symptoms, quarantining those who tested positive but had no or only mild symptoms (the quarantine was monitored using a phone app and strictly enforced), and publicly sharing detailed information about the known incidence of the virus.
A study of 181 cases in China published in the Annals of Internal Medicine found that the mean incubation period for COVID-19 is just over 5 days and only about 1 in 100 cases take longer than 14 days. By implication, if people have been strictly following the guidelines on avoiding contact with others, washing/sanitizing hands, sanitizing other objects, and avoiding hand-to-face contact, it should be possible, after two weeks of lockdown, to identify the vast majority of people who are not infected by testing everyone for the presence of SARS-CoV2 itself.
But that’s a series of big ifs. Since it takes a few days for the virus to replicate in the body to the point at which it is detectable, people who have recently been infected might test negative. Also, it is unlikely to be feasible logistically to test a significant proportion of the population for SARS-CoV2 in a short period of time. Existing tests require the use of RT-PCR, which is expensive and time consuming, not least because it can only be done at a lab, and while the capacity for such tests is increasing, it is likely around 50,000 per day in the entire US.
Test, trace, treat, and isolate may be a feasible option for towns and even cities that currently have relatively low incidence of SARS-CoV2. However, given the lethargic progress of testing in places such as the US, UK and India, and hence poor existing knowledge of the extent of infection, it will not be a universal panacea.
3. Test as many people as possible for the presence of antibodies to SARS-CoV2
Outside those few places that have dramatically ramped up testing, it is likely that many more people have had COVID-19 than have been tested, either because they were asymptomatic or because they did not require clinical attention. Many, perhaps most of those people will no longer have the virus in their system but they should still have antibodies (indicating immunity). In order to identify those people, there should be widespread testing for antibodies to SARS-CoV2.
Antibody tests are inexpensive, quick, and some can be done at home with minimal assistance. Numerous such tests have already been produced or are in development (see the list here). For example, Chinese manufacturer Innovita has produced a test that appears to be effective; in a clinical trial of 447 patients, it identified the presence of antibodies to SARS-CoV2 in 87.3 % of clinically confirmed cases of COVID-19 (i.e. there were approximately 13% false negatives) but zero false positives. Innovita’s test was approved by China’s equivalent of the FDA and has been used widely there.
Scanwell Health, a San Francisco-based startup, has an exclusive license to produce Innovita’s test in the U.S. and has already begun the process for obtaining approval from the US FDA under its Emergency Use Authorization. Scanwell estimates that the total cost of the test, including overnight shipping of the kit and support from a doctor or nurse practitioner from Lemonaid Health, will be around $70. One downside to Scanwell Health’s offering, however, is that it expects it to take 6-8 weeks to begin shipping testing kits once it receives authorization from the FDA.
So far, the FDA has approved at least one SARS-CoV2 antibody test, produced by Aytu Bioscience in Colorado. But Aytu’s test is designed for use by physicians, not at home. In Europe, at least one antibody test, produced by German company PharmactACT, is already available. (That test has similar characteristics to Innovita’s.) Another has been approved by the MHRA in the UK for physician use and is awaiting approval for home use; the UK government has ordered 3.5 million of these tests, with the aim of distributing 250,000 per day by the end of April.
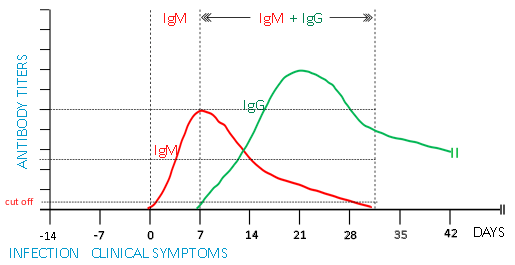
Unfortunately, some people who have antibodies to SARS-CoV2 will also still be infectious. However, because different antibodies develop at different times during the course of infection, it may be possible to distinguish those who are still infectious from those who are no longer infectious. Specifically, immunoglobulin (Ig) M is present in larger amounts while the viral load is still present, while IgG is present in larger amounts later on (see e.g. this and the figure below). So, by testing for the presence of both IgM and IgG it should be possible to identify a large proportion of those who have had COVID-19 but are no longer infectious. (The currently available antibody tests result in about 13 percent false negatives, making them inappropriate as a means of screening out those who do not have COVID-19. But they produce zero false positives, making them ideal for identifying those who definitely have or have had COVID-19). In essence, people whose IgG test is positive but IgM test is negative can then go back to work. In addition, people who have had COVID-19 symptoms, are now symptom-free, and test positive for antibodies, should be allowed to go back to work.
4. Test for SARS-Cov2 among those who test negative for antibodies — and ensure that everyone who tests positive remains in isolation
Those people who test negative for SARS-CoV2 using the quick antibody immunoassay, as well as those who are positive for both IgG and IgM (indicating that they may still be infectious) should then be tested for SARS-CoV2 using the RT-PCR test described above. And those who test negative for SARS-CoV2 should then be permitted to go back to work. But those who test positive should be required to remain in isolation— and seek treatment if necessary.
5. Repeat steps 3 and 4 until nobody tests positive for COVID-19
By repeating steps 3 and 4, it should be possible gradually to enable the vast majority of the population to return to work, and thence to a life of greater normalcy, within a matter of weeks.
6. Some (possibly rather large) caveats
All of this relies on: (a) the ability rapidly to expand testing and (b) widespread compliance with isolation requirements. Neither of these conditions is by any means guaranteed, not least because the rules effectively discriminate in favor of people who have had COVID-19, which may create a perverse incentive to violate not only the isolation requirements but all the recommended hygiene practices — and thereby intentionally become infected with SARS-CoV2 on the presumption that they will then be able to go back to work sooner than otherwise. So, before this is rolled out, it is important to ensure that there will be widespread testing for COVID-19 in a timeframe shorter than the likely total time for contracting and recovering from COVID-19.
In addition, if test results are to be used as a means of establishing a person’s ability to travel and work while others are still under lockdown, it is important that there be a means of verifying the status of individuals. That might be possible through the use of an app, for example; such an app might also provide policymakers to make better resources allocation decisions too.
Also, at-risk individuals should be strongly advised to remain in isolation until there is no further evidence of community transmission.
7. The Mechanics of Testing
Given that there are not currently sufficient tests available for everyone to be tested in most locations, one obvious question is: who should be tested? As noted above, it makes sense initially to target those who have had COVID-19 symptoms and have recovered. Since only those people who have had such symptoms—and possibly their physician if they presented with their symptoms—will know who they are, this will rely largely on trust. (It’s possible that self-reporting apps could help.)
But it may make sense initially to target tests more narrowly. The UK is initially targeting the antibody detection kits to healthcare and other key workers—people who are essential to the continued functioning of the country. That makes sense and could easily be applied in other places.
Assuming that key workers can be supplied with antibody detection kits quickly, distribution should then be opened up more widely. No doubt insurance companies will be making decisions about the purchase of testing kits. Ideally, however, individuals should be able to buy kits such as Scanwell’s without going through a bureaucratic process, whether that be their insurance company or the NHS. And vendors should be free to price kits as they see fit, without worrying about the prospect of being subject to price caps such as those imposed by Medicaid or the VA, which have the perverse effect of incentivising vendors to increase the list price. Finally, in order to increase the supply of tests as rapidly as possible, regulatory agencies should be encouraged to issue emergency approvals as quickly as possible. Having more manufacturers with a diverse array of tests available will increase access to testing more quickly and likely lead to more accurate testing too. Agencies such as the FDA should see this as their absolute priority right now. If the Mayo clinic can compress 6 months’ product development into a month, the FDA can surely do its review far more quickly too. Lives—and the economy—depend upon it.